
From 911 to Hospital: Challenges and Opportunities for AI Integration in Emergency Medical Services
Source: arXiv:2606.16984 · Published 2026-06-15 · By Emily Hou, Marelyn Gonzalez, Andrew L. Kun, Osnat Mokryn, Orit Shaer
TL;DR
This paper investigates the complex challenges and opportunities for integrating AI technologies into Emergency Medical Services (EMS), a high-stakes healthcare domain characterized by distributed teams, dynamic workflows, and extreme time pressure. The authors conduct semi-structured interviews with 25 EMS clinicians across the United States, exploring their current use of technology, cognitive and social coordination mechanisms, and perceptions towards AI integration into their workflows. The study surfaces how EMS work unfolds across ten distinct stages, each with different information needs, constraints, and collaboration patterns, and highlights that AI adoption in EMS is currently limited and fraught with sociotechnical complexity.
The key contribution is an empirical characterization of EMS workflows emphasizing the role of situational awareness (SA) as the fundamental coordination mechanism distributed across team members and artifacts. Participants expressed strong concerns around AI's impact on legal/privacy issues, trust and reliability, contextual sensitivity, professional autonomy, and potential to disrupt tightly coupled communication under stress. The paper proposes five human-centered AI design principles aimed at augmenting distributed cognition and preserving situational awareness and coordination. Overall, it provides a rich, grounded analysis of EMS clinicians’ nuanced attitudes towards AI and outlines sociotechnical design challenges for AI to support, rather than undermine, EMS team effectiveness.
Key findings
- EMS workflow can be divided into 10 stages from dispatch call to hospital handoff, each with distinct information and coordination demands (Sec 4.1).
- EMS clinicians rely on distributed situational awareness across perception, comprehension, and projection levels to coordinate effectively under stress (Sec 2.5).
- AI integration poses threats to SA at all levels: reduced perception via 'out-of-the-loop' attention, opacity weakening comprehension and calibration of trust, and obscured uncertainty harming projection (Sec 2.5.2).
- Concerns raised by EMS clinicians include legal liability, privacy, AI technical reliability, contextual sensitivity, potential workflow friction, and loss of professional autonomy (Sec 4, thematic results).
- Interviews (N=25) reached saturation by the 20th, covering paramedics, EMTs, advanced EMTs, chiefs, from diverse organizational contexts across US municipal, private, and volunteer agencies (Sec 3).
- Strong intercoder reliability (Cohen's κ=0.89) achieved for thematic analysis, enhancing trust in qualitative findings (Sec 3.4).
- Participants envision AI benefits such as improved triage accuracy, enhanced coordination, and training support but emphasize AI must augment rather than replace human SA (Sec 4).
- Five proposed AI design principles emphasize supporting distributed cognition, transparency, respect for autonomy, minimizing workflow disruption, and privacy protections (Sec 5).
Threat model
n/a — This paper focuses on sociotechnical and human factors challenges for AI integration in EMS rather than a traditional security threat model involving adversaries.
Methodology — deep read
Threat Model & Assumptions: The adversary is not explicitly defined since this is a human-computer interaction and sociotechnical study rather than a security evaluation. However, implicit assumptions include EMS workflows under high time pressure and uncertainty, with clinicians vulnerable to reduced situational awareness due to cognitive overload and potential distrust or misuse of AI. The study focuses on frontline EMS clinicians as end users rather than malicious actors.
Data: The qualitative data comprised 25 semi-structured interviews with EMS clinicians across the United States representing diverse roles (paramedics, EMT-b, EMT-a, EMS chiefs), agencies (municipal, private, volunteer), and experience (1–35 years). Interviews lasted 22–63 minutes, conducted June-July 2025 remotely or in person. Transcripts were generated via Otter.ai and manually validated. Data collection ceased after thematic saturation at 20 interviews.
Architecture/Algorithm: Not applicable — this work is qualitative and design-oriented.
Training Regime: Not applicable — qualitative interview study.
Evaluation Protocol: Reflexive thematic analysis was employed. Two coders performed open coding independently, met to reconcile discrepancies, formed a codebook iteratively combining inductive and deductive codes. Coding consistency was assessed on 20% of transcripts with high intercoder reliability (Cohen's κ=0.89). Themes were built through affinity diagramming and contextual interpretation, with attention to empirical grounding and distinction. Saturation analysis was tracked chronologically.
Reproducibility: Data and code are not reported as publicly available, likely to preserve participant confidentiality. The domain expertise of the lead researcher (field EMS experience) was leveraged for interpretive validity but researchers maintained reflexivity to avoid bias.
Concrete example: EMS clinicians described arriving at a scene (stage 3), performing scene size-up to detect hazards (Level 1 SA), integrating cues to comprehend risks (Level 2 SA), and projecting potential patient deterioration (Level 3 SA). They reported how AI tools that do not provide transparent, timely information could disrupt these cognitive processes and coordination, leading to workflow friction and potential errors. For instance, opacity of AI triage recommendations might erode trust or delay critical decisions under acute stress.
Technical innovations
- Empirical characterization of EMS workflows broken down into 10 distinct stages annotated with cognitive, social, and technological factors affecting AI integration.
- Grounding AI design challenges and opportunities within distributed cognition and multi-level situational awareness frameworks tailored to EMS high-pressure contexts.
- Identification of sociotechnical barriers to AI adoption in EMS, including legal/privacy risks, workflow friction, and threats to professional autonomy, derived from frontline clinician voices.
- Proposal of five practical human-centered AI design principles aligned to augment distributed cognition and situational awareness rather than replace clinician expertise.
Datasets
- Interview transcripts from 25 EMS clinicians — approx. 22–63 minutes each — US municipal, private, and volunteer EMS agencies (not publicly released)
Figures from the paper
Figures are reproduced from the source paper for academic discussion. Original copyright: the paper authors. See arXiv:2606.16984.
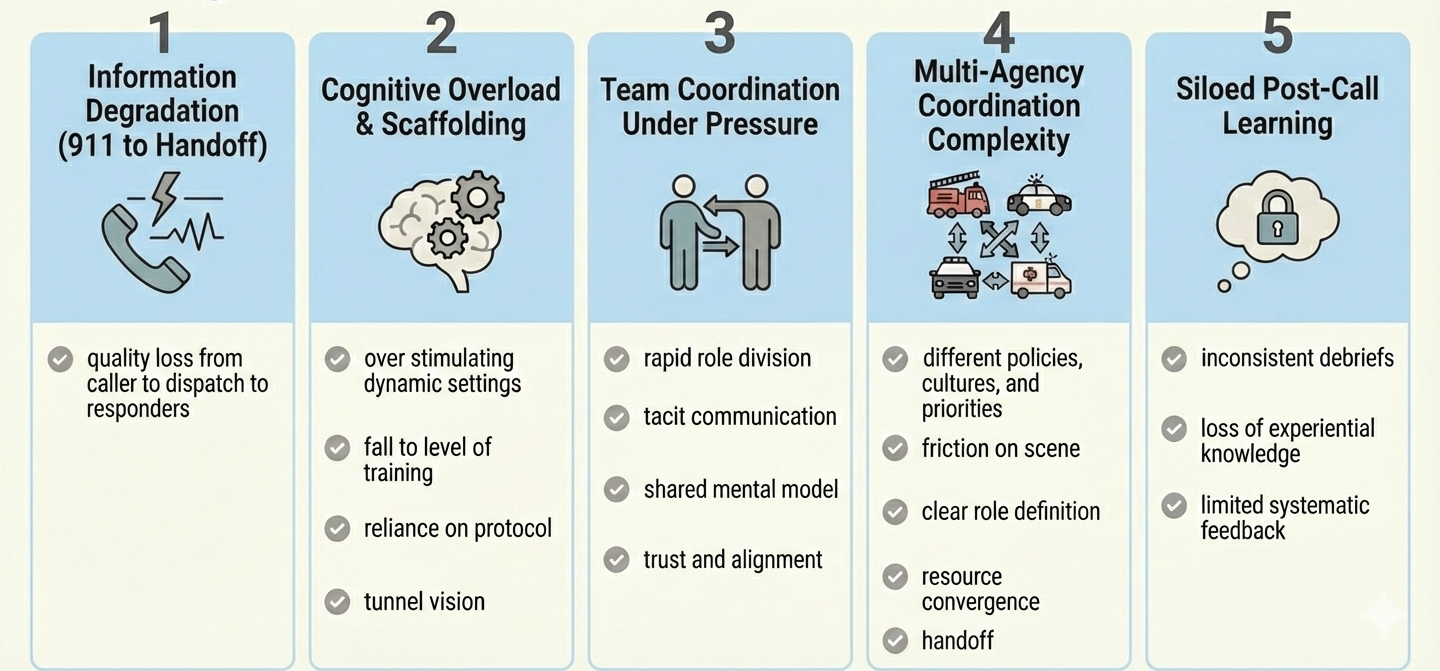
Fig 1: Challenges across the EMS workflow described in
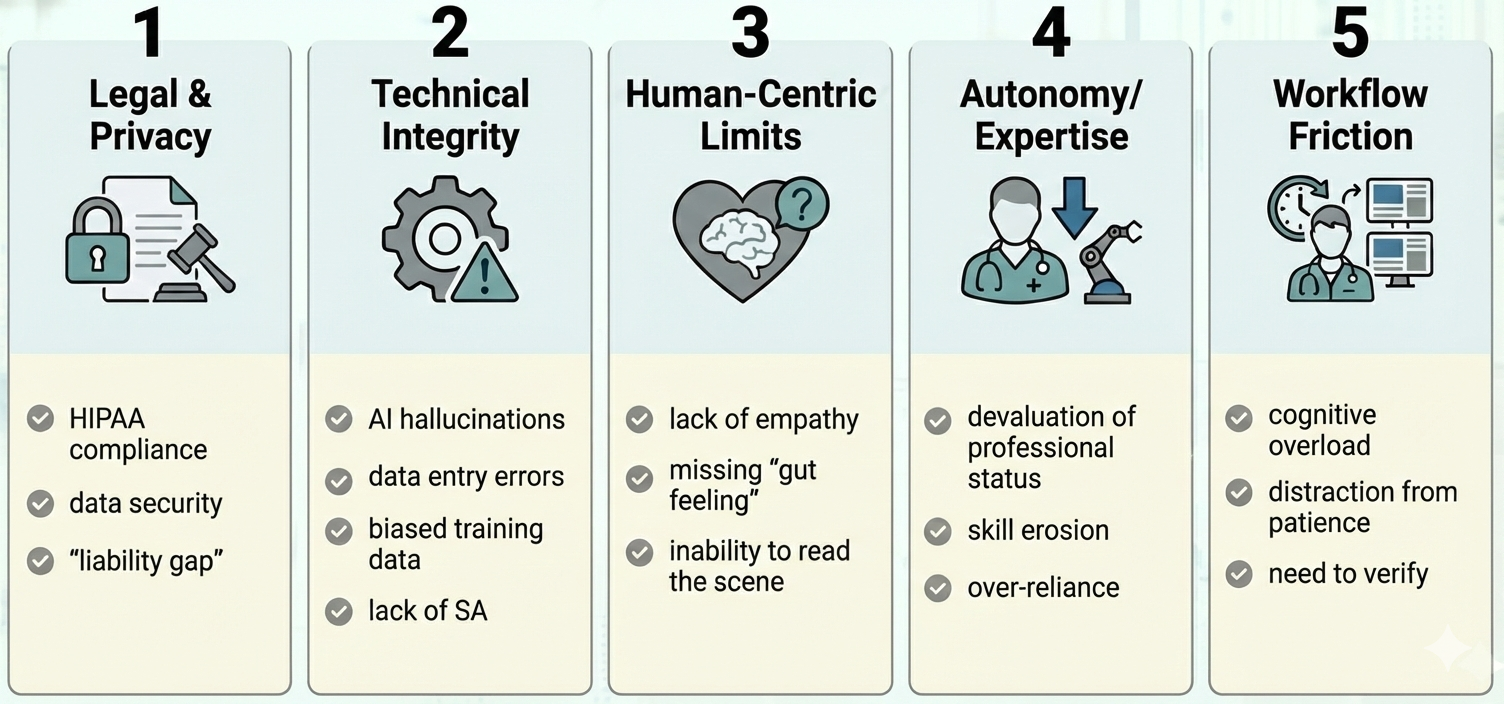
Fig 2: Core tensions of integrating AI into EMS workflows,
Limitations
- Qualitative study with a relatively small sample (N=25) from US EMS systems only; results may not generalize internationally.
- Interviews capture perceptions and self-reported workflow descriptions but lack observational or quantitative behavioral validation.
- No deployment or empirical evaluation of AI tools in EMS contexts; impacts and effectiveness of AI remain speculative.
- Potential bias introduced by the lead interviewer's EMS domain expertise, despite reflexivity efforts.
- Limited consideration of adversarial or malicious use cases of AI in EMS workflows.
Open questions / follow-ons
- How can AI systems be designed to transparently communicate their reasoning and uncertainty to support EMS situational awareness under stress?
- What are effective methods for evaluating real-world AI integration on EMS team coordination, workload, and patient outcomes across workflow stages?
- How might AI impact professional autonomy and legal liability frameworks in EMS, and how can these be addressed proactively?
- How transferable are findings from US EMS contexts to international EMS systems with different structures, resources, and regulations?
Why it matters for bot defense
Bot-defense and CAPTCHA practitioners can draw parallels from this work in understanding how AI augmentation operates within high-stress, distributed human workflows requiring rapid, coordinated decision-making. The research highlights the importance of preserving human situational awareness and trust when integrating AI assistance—not simply aiming for task automation or accuracy gains. For CAPTCHA design and bot-detection, this underscores the value of transparent AI interactions that minimize cognitive disruption, respect user autonomy, and adapt dynamically to contextual signals.
Additionally, the identification of sociotechnical concerns such as workflow friction, privacy/legal issues, and the risks of 'out-of-the-loop' failures when humans rely too passively on AI offers cautionary lessons. Effective bot defense could benefit from mechanisms that maintain human engagement and shared situational awareness rather than replacing human judgment. In practical terms, AI-enabled CAPTCHA systems might consider UI designs that support distributed cognition principles and avoid overwhelming users under time pressure or stress.
Cite
@article{arxiv2606_16984,
title={ From 911 to Hospital: Challenges and Opportunities for AI Integration in Emergency Medical Services },
author={ Emily Hou and Marelyn Gonzalez and Andrew L. Kun and Osnat Mokryn and Orit Shaer },
journal={arXiv preprint arXiv:2606.16984},
year={ 2026 },
url={https://arxiv.org/abs/2606.16984}
}