
Clinical Assistant for Remote Engagement Link (CARE-link): A Web-Based Electronic Health Records Software for Managing Diabetes
Source: arXiv:2606.04952 · Published 2026-06-03 · By Prince Ebenezer Adjei, Joshua Teye Tettey, Toufiq Musah, Audrey Agbeve, John Amuasi
TL;DR
CARE-Link is an open-source, web-based platform designed to improve gestational diabetes management by integrating electronic health records (EHR) with patient-generated data via WhatsApp, mediated by large language models (LLMs). It enables clinicians to aggregate and interpret real-time patient reports outside the clinic, while providing patients with AI-driven personalized guidance and reminders in their own language through a familiar messaging interface. This dual-facing system aims to improve continuity of care, reduce clinician documentation burden, and enhance proactive monitoring in resource-constrained settings, where mobile messaging apps are widely adopted.
The key novelty lies in seamlessly closing the loop between patient chat data and clinical workflows through LLM-assisted summarization, alerting, and AI draft suggestions incorporated into an extensible microservice architecture. The system supports multimodal input (text and speech with local language support) and provides clinicians with contextual, data-driven decision support. Preliminary deployment emphasizes flexibility, security, and scalability, with an architecture designed for adaptation beyond gestational diabetes to other chronic conditions requiring longitudinal tracking and behavior change support.
Key findings
- CARE-Link uses an LLM (ChatGPT API) to analyze WhatsApp patient messages, extract clinical signals, and generate draft visit notes and clinical recommendations that clinicians can review and modify.
- The platform supports multimodal patient input with automatic speech recognition in English and Twi Ghanaian language, enabling broader accessibility across literacy levels.
- AI agents continuously analyze patient-bot conversations to flag priority cases for clinician attention in a dashboard, facilitating early detection of emergencies (e.g., bleeding in late pregnancy).
- Separating the system into microservices (EHR backend in Laravel/PHP and chatbot in Python FastAPI) allows independent scalability and deployment on Azure with encrypted RESTful APIs.
- Clinician-facing dashboard displays structured patient records combined with AI-generated summaries and alerts from real-time patient data, streamlining in-clinic documentation.
- The workflow closes the loop by pushing AI-generated reminders and personalized lifestyle guidance back to patients via WhatsApp at scheduled times, promoting behavioral reinforcement outside visits.
- The modular design permits extensibility by adding new AI agents (e.g., nutrition coach), demonstrated via containerized services integrated through standard JSON/REST APIs.
- All patient data remains in the hospital’s secure cloud tenant; the only external interaction is encrypted prompt text sent to the LLM API, preserving privacy and regulatory compliance (HIPAA/GDPR).
Threat model
Adversaries may attempt to intercept patient-clinician communication or access stored health data but are prevented by end-to-end TLS encryption, role-based access controls, and data residing within secure hospital cloud tenants. The LLM API only receives de-identified prompts, so the system assumes no direct leakage through AI provider channels. The threat model excludes insider attacks with privileged access or advanced LLM prompt injection exploits.
Methodology — deep read
Threat Model & Assumptions: The system assumes adversaries lack access to encrypted communication channels and cannot extract identifiable patient data as all clinical data remain on hospital cloud infrastructure. The LLM provider only receives anonymized prompt text (no direct patient identifiers). The threat model focuses on protecting confidentiality and integrity of sensitive health data exchanged between patient devices, the platform, and clinicians.
Data: Patient data includes demographics, vitals, medical history, obstetric information, lab results, and longitudinal visit records stored in a PostgreSQL database on Azure. Patient-generated health data (PGHD) comprises real-time WhatsApp messages, including text and audio, in English and Twi. Audio undergoes automatic speech recognition before processing. Data is labeled implicitly through clinician input and conversation context rather than pre-labeled datasets. No mention of dataset size or public availability.
Architecture & Algorithm: CARE-Link employs a microservice architecture with decoupled components:
- Web frontend in React for clinicians
- EHR backend in Laravel/PHP handling patient records with PostgreSQL database
- Chatbot service in Python FastAPI processing WhatsApp messages asynchronously
- LLM integration via OpenAI ChatGPT API using domain-specific prompt templates incorporating patient EHR data
- AI agents parse chat logs to extract symptoms, detect emergencies, and pre-fill clinical forms
- The LLM generates personalized patient messages (education, reminders) and clinician recommendations (medication adjustments, lifestyle plans), presented as editable drafts for human oversight.
Training Regime: The paper does not train new AI models; it uses the ChatGPT API as a pre-trained language model. Speech recognition pipelines support local languages. AI agent logic uses prompt engineering rather than explicit machine learning training within CARE-Link.
Evaluation Protocol: The paper does not report formal quantitative evaluation or clinical trials; illustrative use cases demonstrate how AI-generated summaries assist clinicians and how flagged priority cases appear on dashboards. Metrics like accuracy, patient outcomes, or workload reductions are not given. No cross-validation or adversarial testing reported.
Reproducibility: CARE-Link is open-source with public GitHub repository and developer documentation. However, clinical data, LLM API keys, and deployment environment details may limit full reproduction. The system depends on external ChatGPT and WhatsApp Cloud APIs. No frozen weights or benchmark datasets shared.
Example end-to-end workflow: A patient interacts with the WhatsApp chatbot by reporting symptoms via text or voice. The chatbot processes the message via FastAPI service, performing speech recognition if audio, then queries ChatGPT API with contextual patient data to generate an educational reply or to flag red flags. Detected emergency symptoms lead to alerts shown in the clinician dashboard as priority cases. During clinic visits, clinicians open the patient record with AI-suggested summaries pre-filled from patient chats, which they can edit. After clinician updates, new treatment plans and reminder schedules are stored and pushed back to the patient chatbot for ongoing engagement. This cycle enables continuous remote monitoring and contextualized clinical decisions.
Technical innovations
- Closed-loop integration of patient-generated health data via WhatsApp with EHR workflows mediated by LLMs, enabling real-time bidirectional AI assistance.
- Multimodal AI chatbot supporting both text and local-language speech inputs through integrated automatic speech recognition (ASR).
- An AI conversation analyzer agent that automatically extracts clinical signals from patient-chat logs and pre-fills clinical record fields to reduce documentation burden.
- Modular, microservice architecture separating chatbot and EHR services allowing scalable, secure deployment and extensibility with additional AI agents.
Figures from the paper
Figures are reproduced from the source paper for academic discussion. Original copyright: the paper authors. See arXiv:2606.04952.
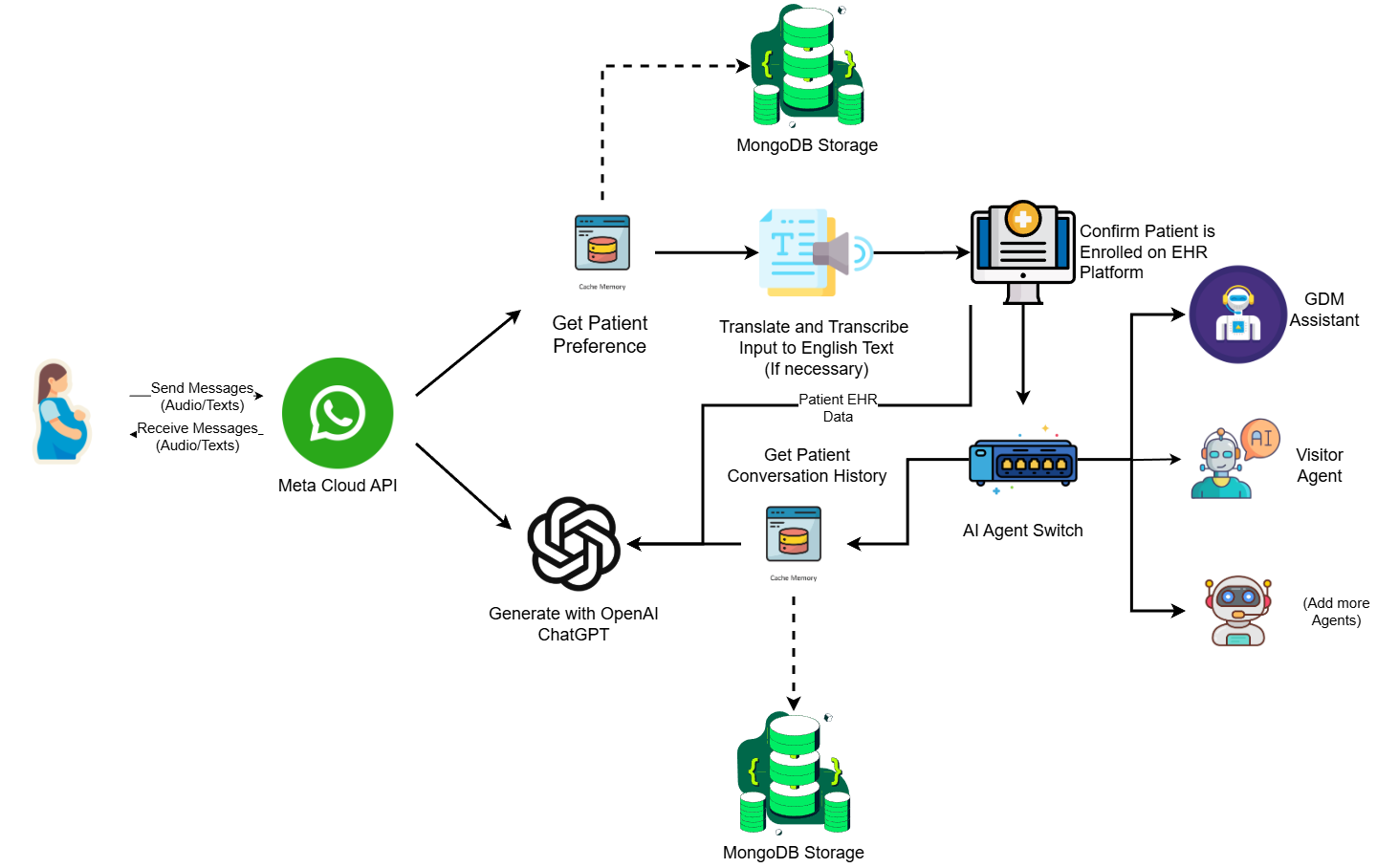
Fig 1: Illustrates the end-to-end data flow and microservice interactions underlying the CARE-
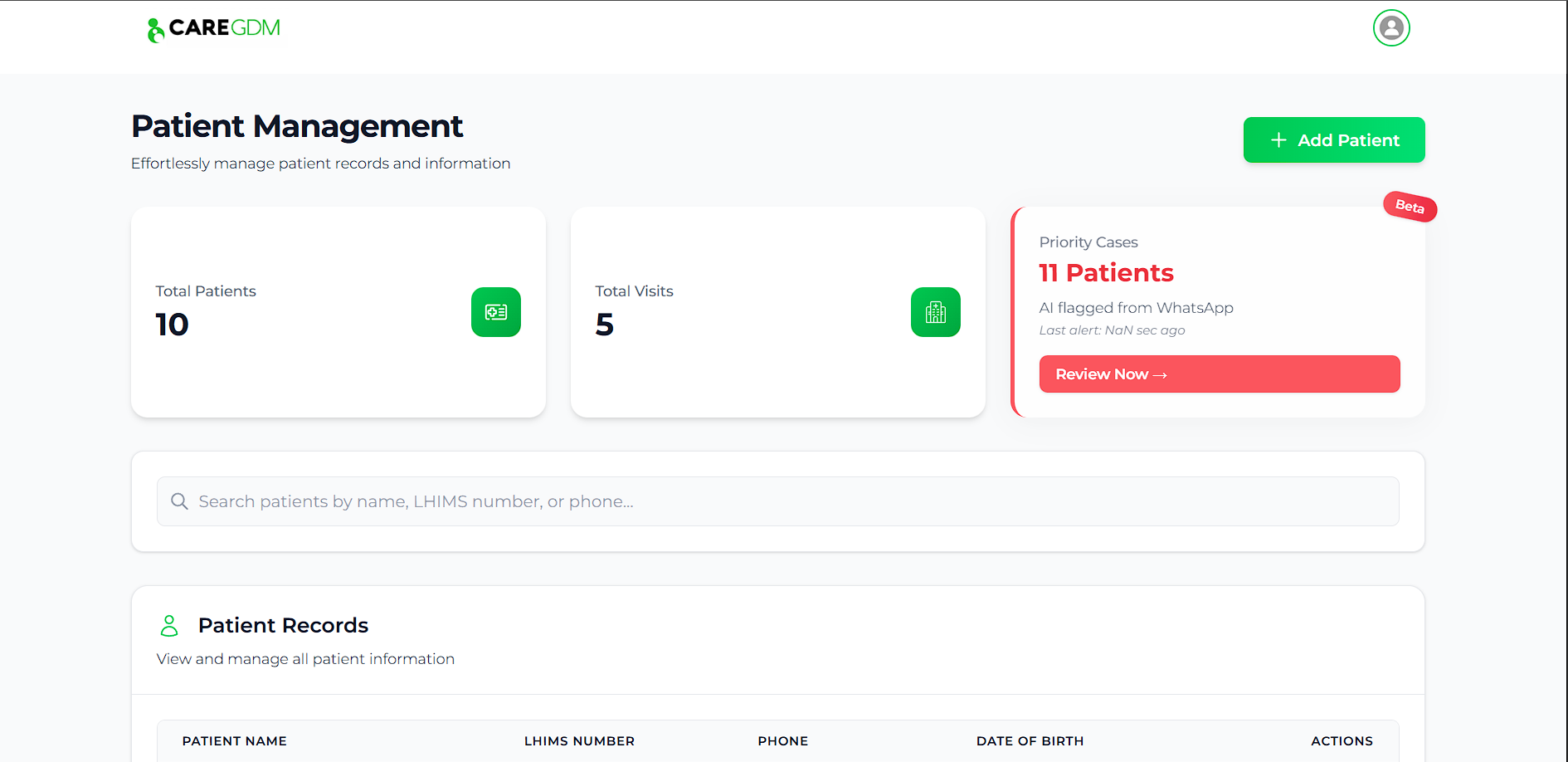
Fig 2: Page showing details of example emergency cases flagged by the agent
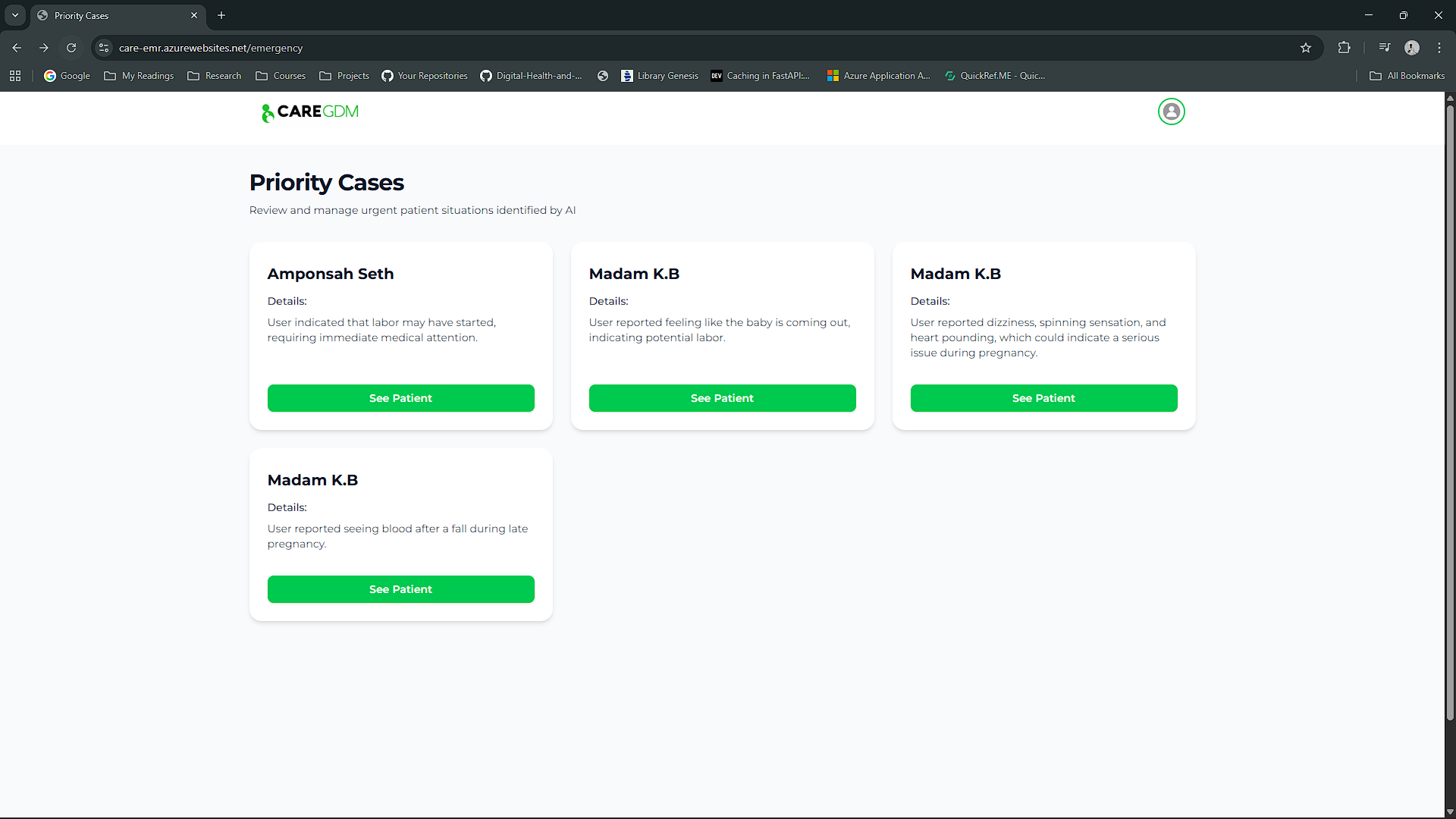
Fig 3: Add New Record Interface
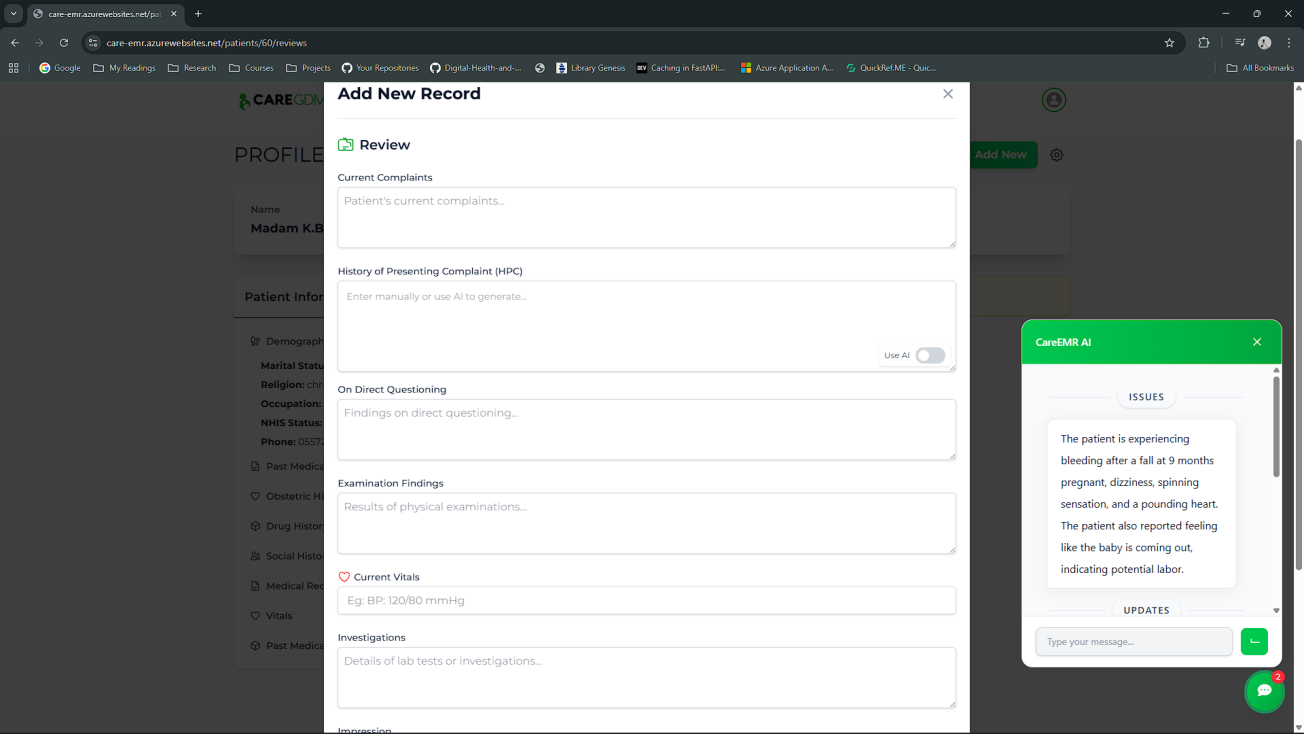
Fig 5: Panels (a) and (b) illustrate bidirectional message exchanges between the patient and
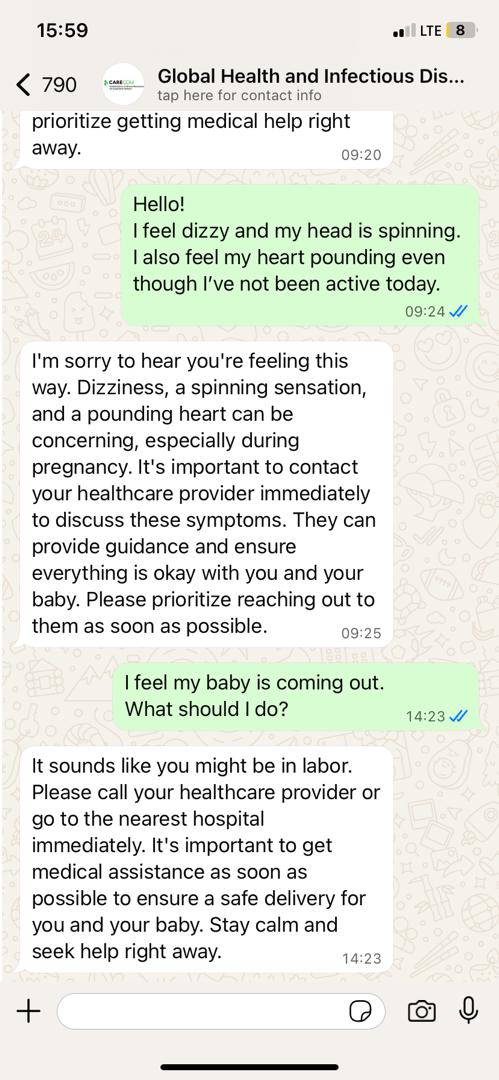
Fig 5 (page 7).
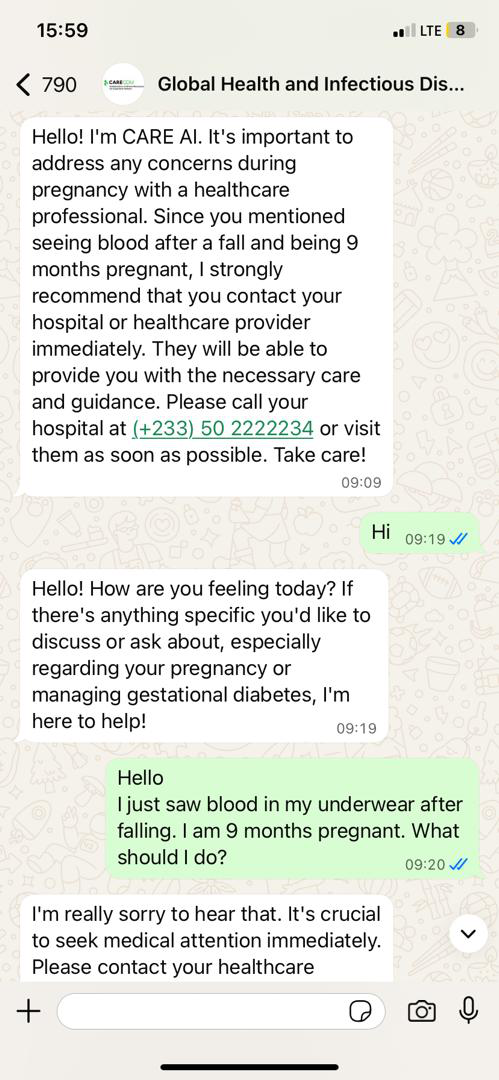
Fig 6 (page 7).
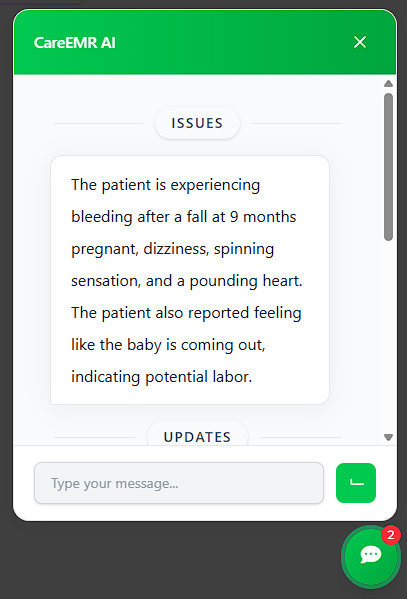
Fig 7 (page 8).
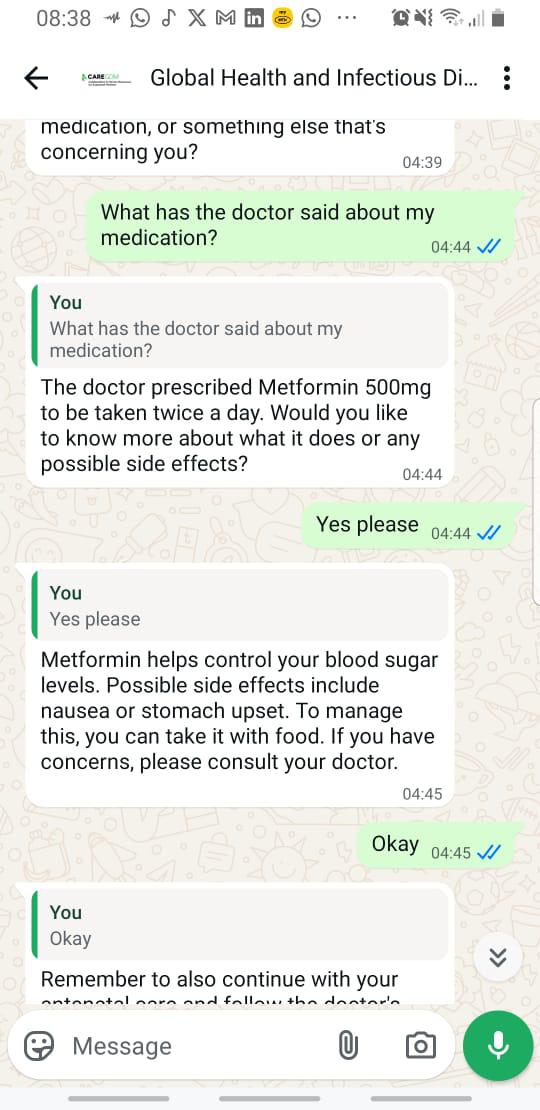
Fig 8 (page 8).
Limitations
- No quantitative evaluation or clinical trial data presented to validate efficacy, patient outcomes, or clinician workload reductions.
- Dependency on external proprietary APIs (OpenAI ChatGPT, WhatsApp Cloud) raises concerns about data privacy, cost, and API availability.
- System deployment described for gestational diabetes; generalizability to other chronic diseases remains to be demonstrated.
- No adversarial robustness analysis or security evaluation of AI-generated content or potential hallucinations by LLM.
- Non-public clinical data and lack of dataset details limit external reproducibility and benchmarking.
- Local language support currently limited to Twi; broader language coverage and cultural adaptation require further work.
Open questions / follow-ons
- What is the measurable impact of LLM-mediated clinical assistants on patient adherence, glycemic control, and maternal/foetal outcomes in real-world trials?
- How does embedding AI chatbots within WhatsApp affect patient-clinician trust, engagement, and perceptions of empathy?
- Which design and governance strategies best mitigate risks from LLM hallucinations or incorrect clinical suggestions?
- What are optimal financial and operational models to sustain AI-powered digital health tools in low-resource settings?
Why it matters for bot defense
From a bot-defense perspective, CARE-Link illustrates a mature use case of AI-mediated bi-directional messaging systems integrated with personal health data. The system relies on trusted APIs and secure communications to safely process sensitive patient messages and generate context-aware responses without leaking privacy. Bot-defense engineers should note the architectural benefits of microservices separation, strict role-based access, encrypted transports, and audit logging when deploying conversational agents in regulated environments. The use of a familiar messaging platform (WhatsApp) for patient interaction also shows practical tradeoffs between user accessibility and security controls. However, the system does not specifically address adversarial attempts to game or spoof the AI chatbot, which is a gap relevant for bot-detection in conversational AI deployments. Overall, CARE-Link serves as a benchmark for integrating large language models with critical real-world health workflows in an extensible, privacy-conscious manner, demonstrating promising architectural patterns for similar AI-assisted bot scenarios requiring sensitive information handling and closed-loop human oversight.
Cite
@article{arxiv2606_04952,
title={ Clinical Assistant for Remote Engagement Link (CARE-link): A Web-Based Electronic Health Records Software for Managing Diabetes },
author={ Prince Ebenezer Adjei and Joshua Teye Tettey and Toufiq Musah and Audrey Agbeve and John Amuasi },
journal={arXiv preprint arXiv:2606.04952},
year={ 2026 },
url={https://arxiv.org/abs/2606.04952}
}