
CogAdapt: Transferring Clinical ECG Foundation Models to Wearable Cognitive Load Assessment via Lead Adaptation
Source: arXiv:2605.22774 · Published 2026-05-21 · By Amir Mousavi, Mohammad Sadegh Sirjani, Erfan Nourbakhsh, Mimi Xie, Rocky Slavin, Leslie Neely et al.
TL;DR
This paper addresses the challenge of real-time cognitive load assessment using wearable ECG devices, which are limited by sparse lead configurations and small labeled datasets. Existing ECG foundation models pretrained on large clinical 12-lead data achieve rich ECG representations but cannot be applied directly to wearables due to sensor configuration mismatch and task differences. The authors propose CogAdapt, a framework that adapts clinical ECG foundation models to wearable cognitive load classification by bridging 3-lead wearable signals to 12-lead clinical format with a novel LeadBridge adapter and progressively fine-tuning the pretrained encoder using ProFine to prevent catastrophic forgetting. Evaluations on two public datasets (CLARE, CL-Drive) under leave-one-subject-out cross-validation demonstrate substantial performance improvements, with macro-F1 increasing from 0.514 and 0.607 (training from scratch) to 0.626 and 0.768 respectively for CogAdapt's full fine-tuning scenario. The results validate transferring large-scale clinical ECG knowledge to wearable cognitive load tasks as a promising direction for robust subject-independent assessment.
Key findings
- CogAdapt (full fine-tuning, Scenario C) improves LOSO macro-F1 from 0.514 to 0.626 on CLARE and from 0.607 to 0.768 on CL-Drive compared to training models from scratch.
- Macro-F1 under less stringent 10-fold cross-validation also improves, reaching 0.785 (CLARE) and 0.860 (CL-Drive) with CogAdapt Scenario C.
- AUROC rises substantially under LOSO with Scenario C, e.g. CLARE AUROC increases from 0.539 to 0.799, indicating better class ranking beyond accuracy.
- LeadBridge adapter achieves near-perfect reconstruction for 7 limb leads and lowest RMSE among baselines for 4 of 5 precordial leads (V2–V5), with +22.5% relative correlation coefficient gain on V2 lead over linear regression and Dower transforms on PTB-XL dataset.
- Progressive fine-tuning via ProFine progressively unfreezing layers (Scenario A to C) correlates with monotonic performance gains; partial unfreeze (Scenario B) lifts LOSO macro-F1 on CL-Drive from 0.578 to 0.704.
- LeadBridge's data-driven 3→12 lead mapping handles wearable sensor placement variability better than fixed mathematical transforms.
- Window-wise normalization and WCT re-referencing minimize covariate shift and prevent data leakage during evaluation.
- Task-specific end-to-end fine-tuning after pretraining the adapter on clinical sinus rhythm data further improves generalization for cognitive load classification.
Threat model
n/a — This work focuses on applying transfer learning techniques to adapt clinical ECG foundation models for wearable cognitive load assessment rather than on security or adversarial threat models.
Methodology — deep read
The paper's methodology proceeds as follows:
Threat Model & Assumptions: The adversary is not explicitly defined since this is a biosignal transfer learning study; the primary challenge is domain shift between clinical 12-lead ECGs and wearable 3-lead devices, plus task shift from cardiac diagnosis to cognitive load assessment. No adversarial perturbations or spoofing attacks are considered.
Data: Three datasets are critical:
- PTB-XL: 21,837 clinical 12-lead ECGs used to pretrain the LeadBridge adapter on normal sinus rhythm samples (approx. 9,500 examples).
- CLARE: 3-lead wearable ECG from 20 subjects performing cognitive tasks, with self-reported cognitive load labels every 10s.
- CL-Drive: 3-lead wearable ECG from 21 drivers with 10s cognitive load labels in simulated driving. Signals resampled to 500Hz, bandpass filtered (0.5-40 Hz), segmented into 5-second windows with 50% overlap for training. Labels binarized (load 1-4 = low, 5-9 = high).
- Architecture & Algorithms: CogAdapt pipeline consists of:
- Data Processing with WCT re-referencing (transforming wearable leads relative to Wilson Central Terminal), windowing, and per-window z-score normalization.
- LeadBridge Adapter: A three-layer Conv1D network (64,64,12 output channels with batch norm and ReLU) that maps 3-lead input to 12-lead output. Pretrained on PTB-XL normal sinus rhythm data to reconstruct clinical leads, initialized with Kaiming, refined end-to-end during downstream training.
- ECG-FM Encoder: A 91M-parameter transformer pretrained on 1.5 million clinical 12-lead ECGs to produce 768-D embeddings.
- Classification Head: Lightweight 1D CNN (three convolutional layers projecting pooled embeddings) trained to classify cognitive load with focal loss for class imbalance handling.
- Training Regime: The ProFine progressive fine-tuning strategy has three scenarios:
- Scenario A: Freeze encoder, train only LeadBridge and classifier with data augmentation and focal loss.
- Scenario B: Partial unfreeze of top 2 encoder layers + adapter + head; cross-entropy loss.
- Scenario C: Full fine-tuning of encoder + adapter + head with layer-wise learning rate decay, no augmentation, cross-entropy loss. Training uses AdamW optimizer, early stopping on validation macro-F1 (LOSO) or AUROC (k-fold), batch sizes and epoch counts not explicitly detailed. Class weights computed to rebalance loss.
- Evaluation Protocol: Two validation schemes:
- LOSO (leave-one-subject-out) cross-validation to measure generalization across unseen subjects, the primary evaluation setting.
- 10-fold stratified cross-validation as less stringent baseline. Metrics reported include accuracy, macro-F1, and AUROC. Baselines include training LightCNN and Transformer from scratch on same 3-lead inputs. Statistical significance testing is not mentioned.
- Reproducibility: Code release or pretrained weights are not specified. Datasets CLARE and CL-Drive are public; PTB-XL is well-known.
Concrete Example End-to-End: A 5-second ECG window from CLARE wearable leads is preprocessed and WCT-referenced, then passed through LeadBridge which converts 3 leads to synthetic 12-lead signals aligned with clinical lead distributions. This output feeds into the frozen or fine-tuned ECG-FM transformer encoder, producing a pooled embedding vector. The lightweight CNN head classifies this embedding to low vs high cognitive load, minimizing focal or cross-entropy loss depending on scenario. Progressive fine-tuning adjusts encoder weights stepwise to adapt clinical ECG representations to subtle autonomic nervous system variations indicative of cognitive load.
Technical innovations
- LeadBridge: A learnable convolutional adapter transforming 3-lead wearable ECG signals into anatomically consistent 12-lead representations for compatibility with clinical ECG foundation encoders, pretrained on PTB-XL and refined end-to-end.
- ProFine: A progressive fine-tuning strategy that gradually unfreezes ECG-FM transformer encoder layers with layer-wise learning rate decay to balance plasticity for task adaptation against catastrophic forgetting.
- Application of Wilson Central Terminal re-referencing and window-wise normalization to reduce domain shift between wearable and clinical ECG signals prior to adaptation.
- End-to-end task-specific adapter refinement that prioritizes cognitive load classification performance over pure lead reconstruction fidelity.
Datasets
- PTB-XL — 21,837 clinical 12-lead ECGs — public clinical dataset for lead reconstruction pretraining
- CLARE — 20 subjects, wearable 3-lead ECG with 10s cognitive load self-reports — public wearable cognitive load dataset
- CL-Drive — 21 subjects, wearable 3-lead ECG with 10s cognitive load labels during simulated driving — public wearable cognitive load dataset
Baselines vs proposed
- ECG-LightCNN (CLARE LOSO macro-F1): 0.514 vs CogAdapt Scenario C: 0.626
- ECG-LightCNN (CL-Drive LOSO macro-F1): 0.607 vs CogAdapt Scenario C: 0.768
- Transformer (CLARE LOSO macro-F1): 0.496 vs CogAdapt Scenario C: 0.626
- Transformer (CL-Drive LOSO macro-F1): 0.541 vs CogAdapt Scenario C: 0.768
- LeadBridge vs Dower inverse transform (V2 RMSE): 175.61 vs 205.69 (lower is better)
- LeadBridge vs Linear regression (V2 RMSE): 175.61 vs 195.08
- LeadBridge vs Dower transform (V2 Correlation Coefficient): 0.669 vs 0.546
Figures from the paper
Figures are reproduced from the source paper for academic discussion. Original copyright: the paper authors. See arXiv:2605.22774.
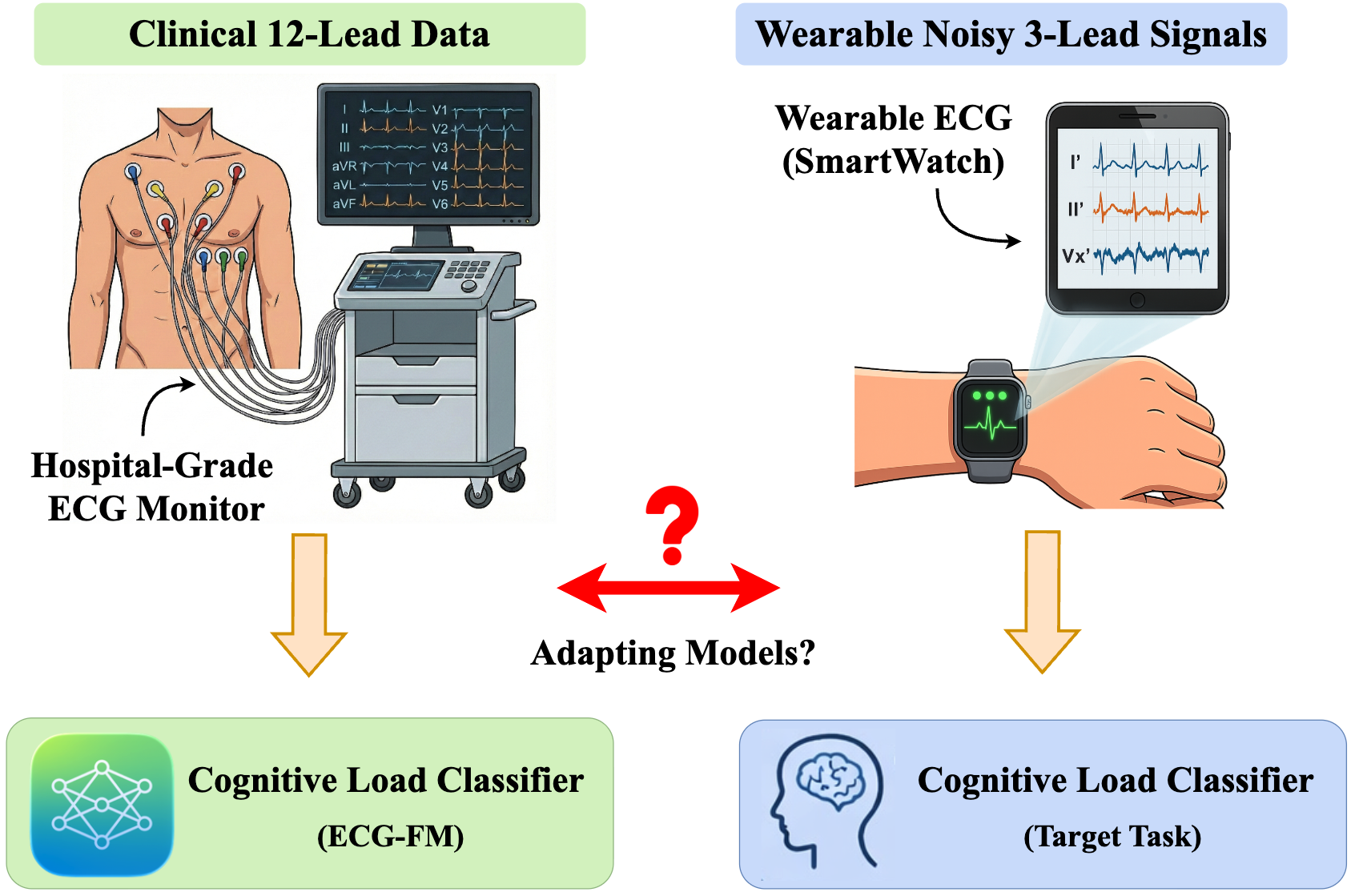
Fig 1: The core challenge: Pre-trained foundation models expect
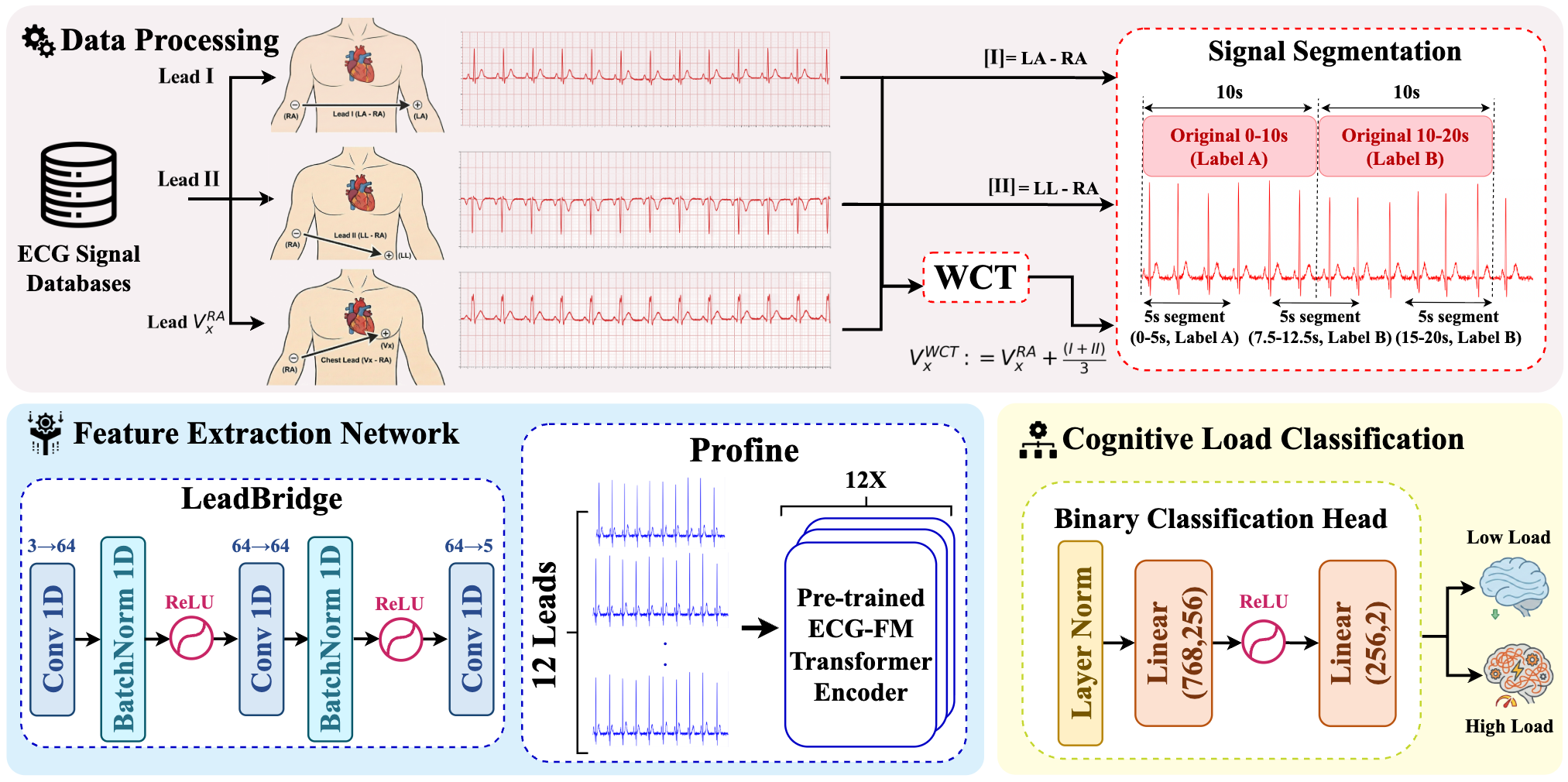
Fig 2: CogAdapt architecture bridging wearable 3-lead ECG to clinical 12-lead foundation models. The framework consists of data
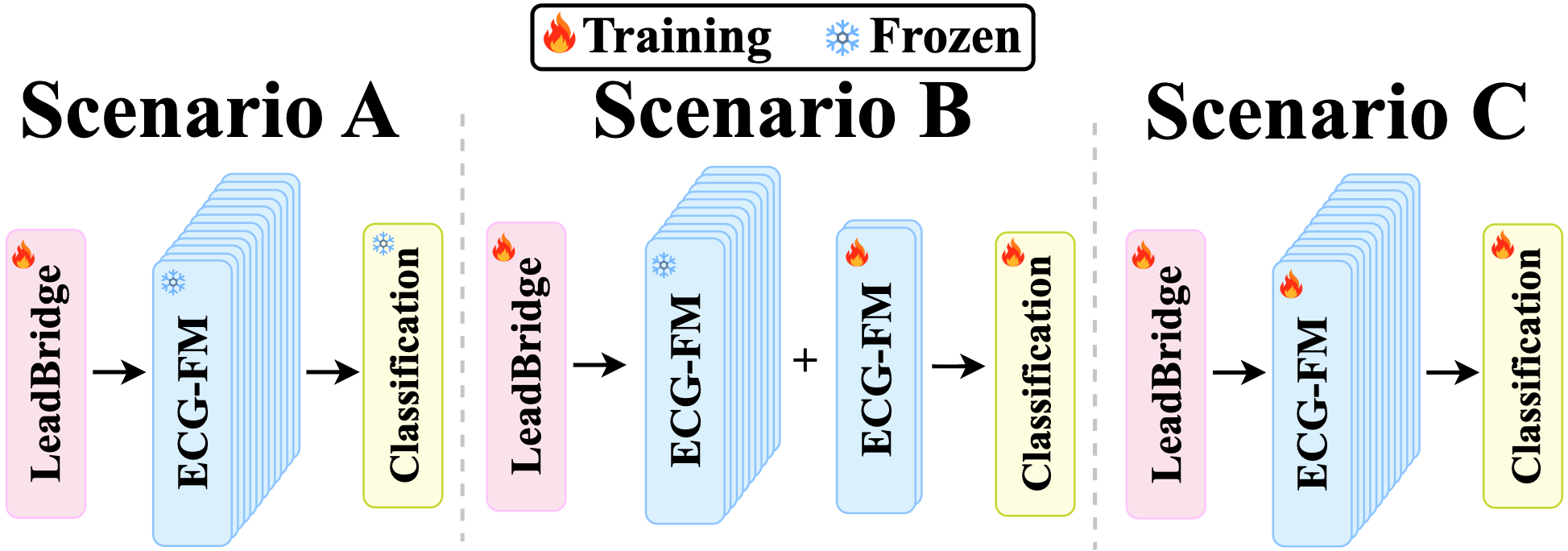
Fig 3: Progressive fine-tuning scenarios.
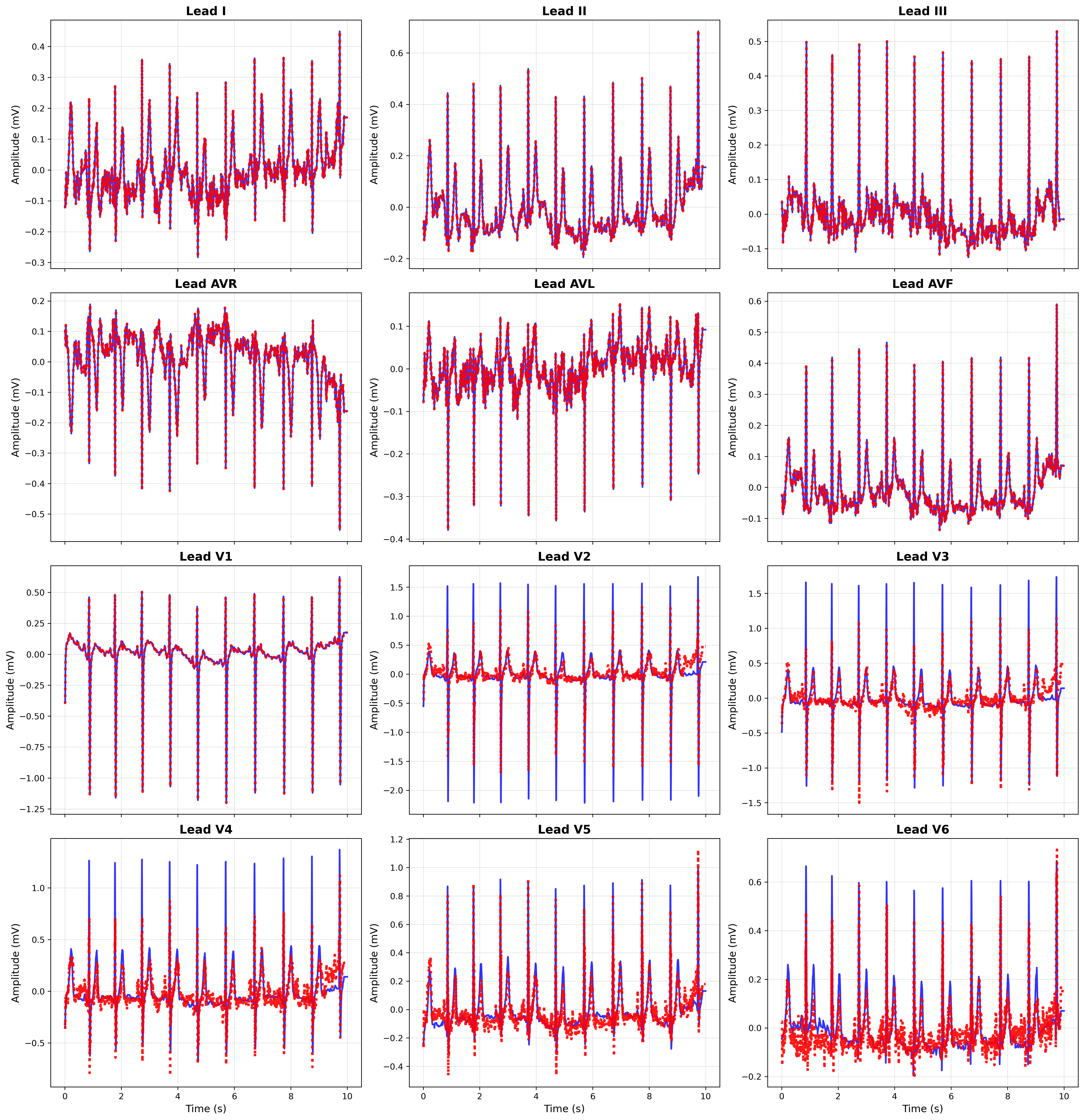
Fig 4: ECG lead reconstruction on PTB-XL. Reconstructions of
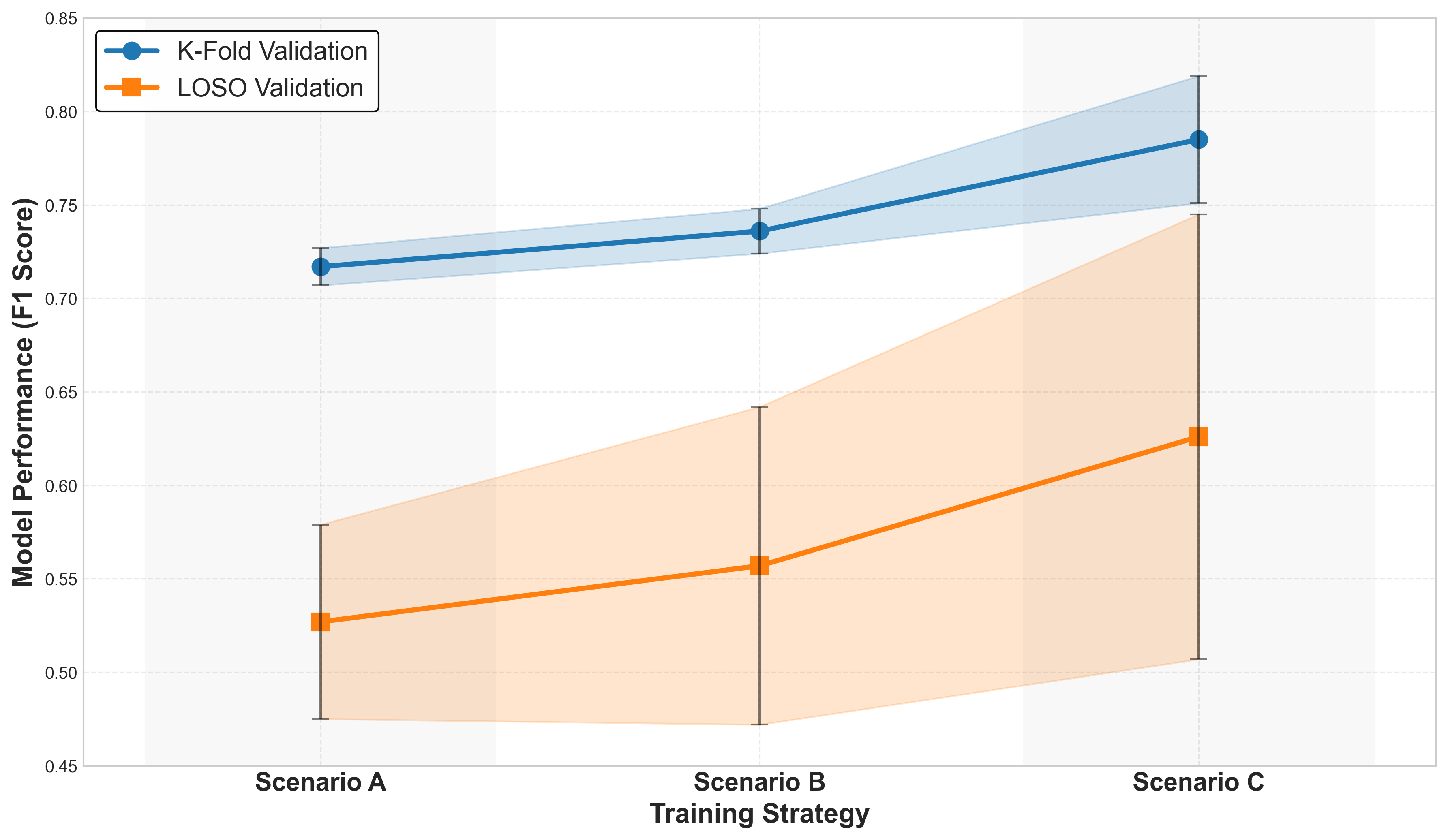
Fig 5: Plasticity–stability trade-off for CLARE dataset across
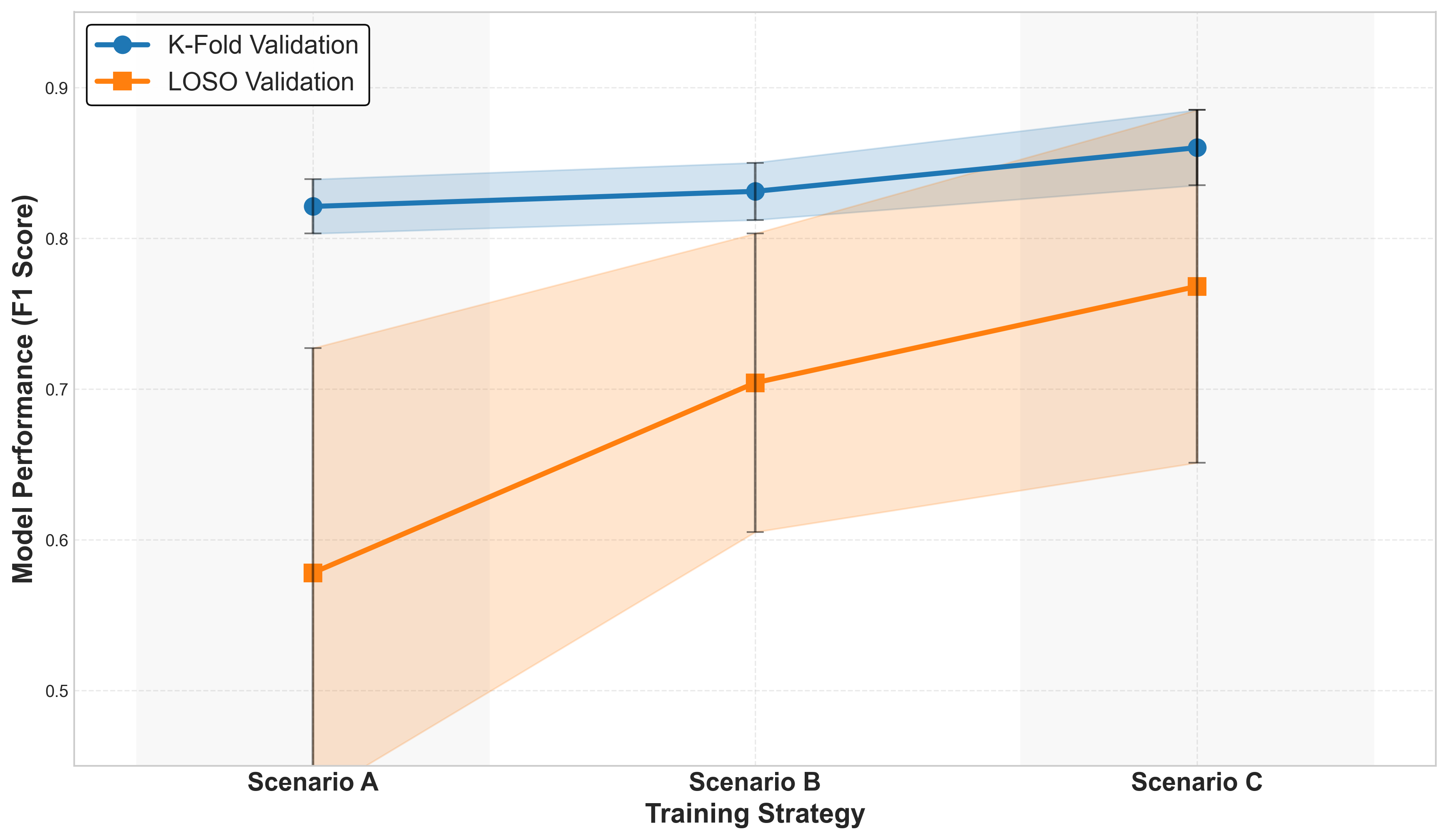
Fig 6: Plasticity–stability trade-off for CL-DRIVE dataset across
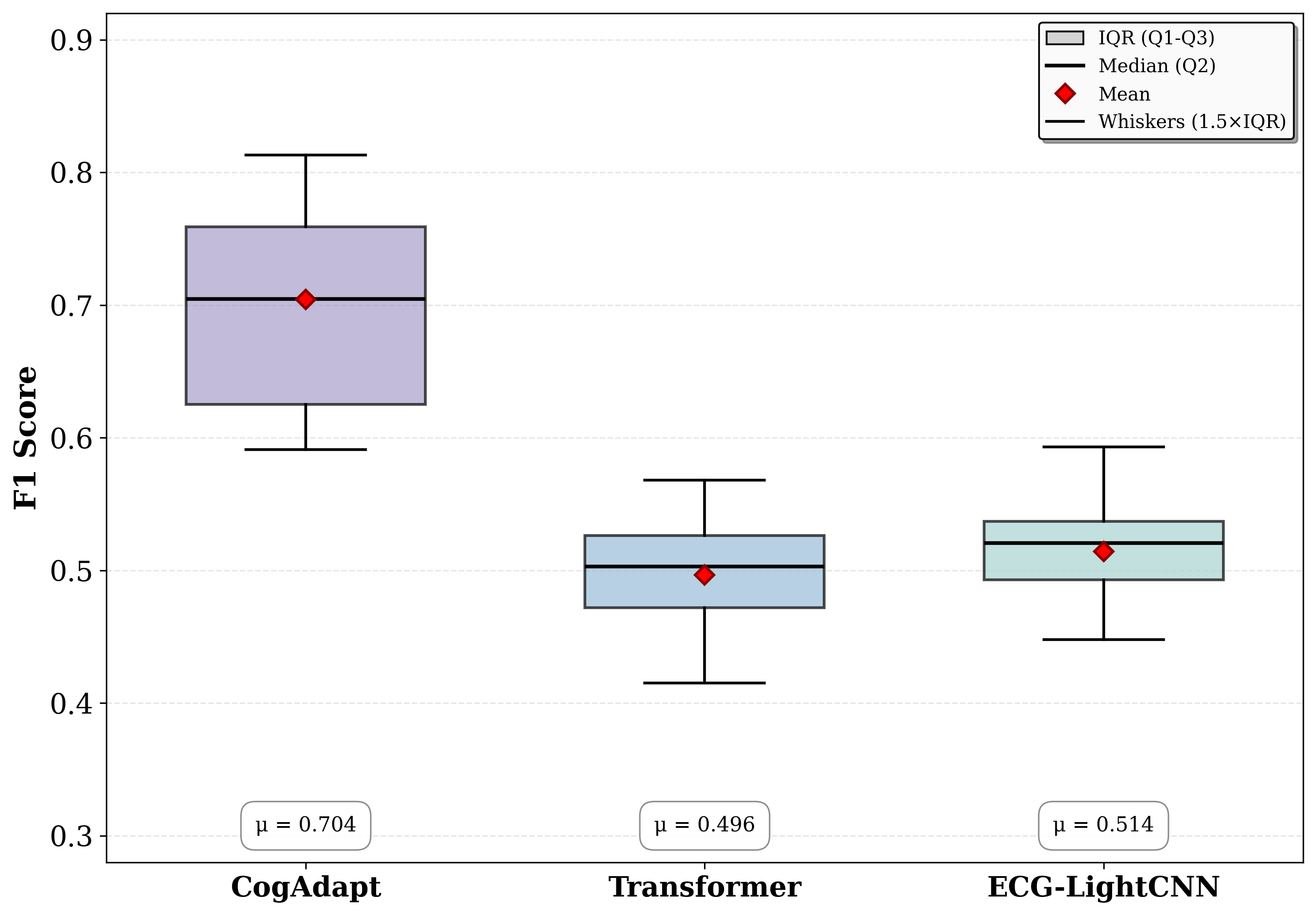
Fig 8: Per-subject accuracy across all training stages under LOSO cross-validation on the CLARE dataset.
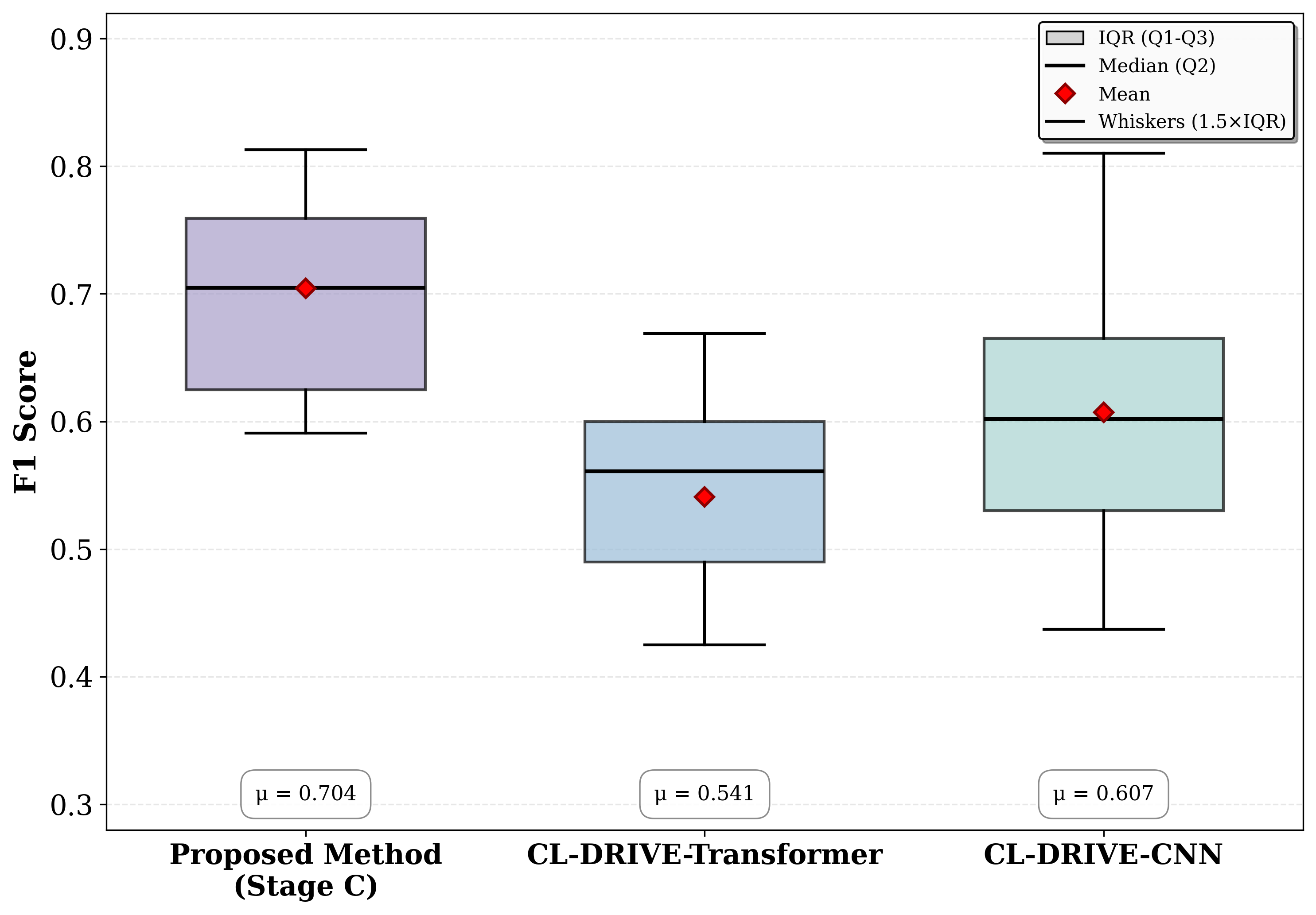
Fig 10: Performance distribution comparison on CL-Drive
Limitations
- Limited number of subjects (20-21) and recording hours in wearable cognitive load datasets constrain robustness and generalization testing.
- No explicit adversarial evaluation or testing against sensor noise beyond standard augmentations.
- The adapter pretraining assumes normal sinus rhythm ECGs and may not generalize to pathological cardiac conditions in wearables.
- Progressive fine-tuning hyperparameters and exact training budgets are not exhaustively detailed; reproducibility depends on these unstated details.
- No ablation analysis explicitly isolates impacts of WCT re-referencing versus LeadBridge versus normalization separately.
- External validation on truly out-of-distribution wearable devices or real-world ecological data is not performed.
Open questions / follow-ons
- How well does the LeadBridge adapter generalize to wearable devices with different lead placement schemes beyond those in CLARE and CL-Drive?
- Can the proposed framework accommodate multi-modal physiological signals jointly (e.g., combining ECG with motion or respiration signals) for improved cognitive load modeling?
- What are the trade-offs and data efficiency gains of semi-supervised or few-shot personalization of CogAdapt to individual subjects with minimal calibration data?
- How does the framework perform under real-world conditions with motion artifacts, electrode detachment, or low signal-to-noise ratios compared to controlled datasets?
Why it matters for bot defense
Bot defense and CAPTCHA systems increasingly capitalize on physiological signals for user authentication and intent detection. CogAdapt’s approach to transferring large-scale clinical ECG foundation models to wearable sensor data via learnable lead adaptation and progressive fine-tuning addresses core domain mismatch and data scarcity issues relevant for such biometric and behavioral analysis. The methodology demonstrates that deep models pretrained on standardized, rich datasets can be adapted to noisier, lower-fidelity wearable signals while maintaining subject-independent performance. While cognitive load classification differs from bot detection tasks, the paper’s domain transfer techniques and adapter design principles could inspire CAPTCHA practitioners working with biosignals or any modality with sensor layout mismatch. Understanding stable finite-dimensional transformations that preserve task-relevant signal morphology while reducing domain gaps is broadly applicable. However, the focus here is on physiological signal classification rather than adversarial attack resilience or spoofing defense, so direct bot-detection security implications are limited. Practitioners may consider modular adapter layers and progressive fine-tuning strategies to improve cross-device and cross-subject generalization challenges typical in biometrics and behavior-based bot-defense.
Cite
@article{arxiv2605_22774,
title={ CogAdapt: Transferring Clinical ECG Foundation Models to Wearable Cognitive Load Assessment via Lead Adaptation },
author={ Amir Mousavi and Mohammad Sadegh Sirjani and Erfan Nourbakhsh and Mimi Xie and Rocky Slavin and Leslie Neely and John Davis and John Quarles },
journal={arXiv preprint arXiv:2605.22774},
year={ 2026 },
url={https://arxiv.org/abs/2605.22774}
}